

INTRODUCTION
Cigarette smoking is one of the most serious public health issues in the world. It is associated with the development of a variety of diseases, including lung, throat, oral, bladder, cervical, liver, kidney, pancreatic cancer, chronic obstructive pulmonary disease, and cardiovascular disease1. Smoking is one of the main causes of death worldwide. Globally, tobacco use kills approximately 7 million people a year and increases susceptibility to six of the eight common causes of death2.
The total tobacco-attributable deaths are projected to rise from 5.4 million in 2005 to 6.4 million in 2015 and 8.3 million in 20303, with an estimated 600000 deaths attributable to secondhand smoke4. These projections are based on models that show a three- to four-decade lag between the rise in smoking prevalence and the resulting increase in smoking-attributable mortality5. A 50-year study found that smokers live about 10 years less than non-smokers, and according to this recent scientific research, even though smoking is harmful to the people around smokers and at risk of lung cancer and other diseases6, the enormous health and economic costs of the smoking epidemic are likely to increase in future decades7.
In 2012, an estimated 928 million men and 207 million women were current smokers8. In 2021, over 1.3 billion people worldwide were estimated to be cigarette smokers, 80% of whom live in low- and middle-income countries2. In general, East and Southeast Asia and Eastern Europe currently have the highest male smoking prevalence rates. North and South America, Oceania, and the European nations have the highest rates of female smokers9.
There is a significant difference in trends in smoking prevalence among countries, and worldwide, cigarette consumption is rising at about 3% yearly10,11. While many countries, notably high-income countries, have seen a considerable decrease in smoking prevalence among both males and females, in many other nations, there has been little decrease or even an increase in smoking prevalence12. In Asia, Southern and Eastern Europe, and developing countries, tobacco use is increasing at about 8% per year. Yet, in some industrialized countries, smoking rates are decreasing at about 1% a year, largely due to the implementation of significant anti-tobacco programs. As with all other epidemics involving a major behavioral component, the exact timing, duration, and magnitude of the smoking epidemic varies significantly from one country to another10. In Iran, a country neighboring Iraq, around 20% of males and 2% of females smoke tobacco products13. A number of limited studies were conducted14-16. A study conducted in Iraq in 2012 in preparatory and secondary schools in Baghdad showed that the 21.8% of Iraqi adolescents (male 27.1%, female 12.7%) are tobacco users17.
Because of insufficient data and a lack of literature on the smoking prevalence in Iraq, this study aimed to identify the smoking prevalence among males and females in the Iraqi population.
METHODS
Design and participants
In this cross-sectional study, a questionnaire survey was carried out between August and November 2021 in the 19 provinces of Iraq using a descriptive cross-sectional methodology, using a convenience sample of Iraqi adults. We utilized an online survey questionnaire. The link of the questionnaire was shared across Iraq mostly via social media. Informed consent was obtained from all respondents through a detailed cover letter, which included instructions, explained the purpose of the study, assured confidentiality, and confirmed that participation was voluntary. Respondents provided their consent by agreeing to proceed with the survey after reading this information. The protocol was approved by the Ethics Licensing Committee of the Kalar Technical College at the Sulaimani Polytechnic University (No.06 on 5 July 2021) and followed the Declaration of Helsinki.
Questionnaire and data collection
The questionnaire was a web-based system and was in the main Iraqi languages, Arabic and Kurdish (Kurdish-Sorani and Kurdish-Kirmanji), for ease of comprehension. The questionnaire had two sections with six questions each that focused on the goals of the study. Section one collected demographic data on age, gender, and residence; and Section two collected data on smoking, and included the questions: ‘Do you smoke cigarettes?’, ‘What is the number of cigarettes you smoke per day?’, and ‘What is the period of your smoking habit in years?’.
We gathered and extracted all six responses for all participants to an Excel sheet in the application’s database layer. We used ASP.NET for its front end and SQL Server for its data warehouse18. Those who failed to completely fill in the questionnaire were excluded, while duplicate entries were rejected by the system through the use of the HTTP Cookie class of C# programming.
RESULTS
In total 13142 participants of different race, age, and gender from all of the Iraqi provinces participated in the study (Supplementary file Table 1). The smoking rate of the study population of 13142 people (8815 males and 4327 females) was 22.44% (2949 people; 2795 males and 154 females). The smoking rate of males at 31.7% was significantly higher than that of females at 3.6%.
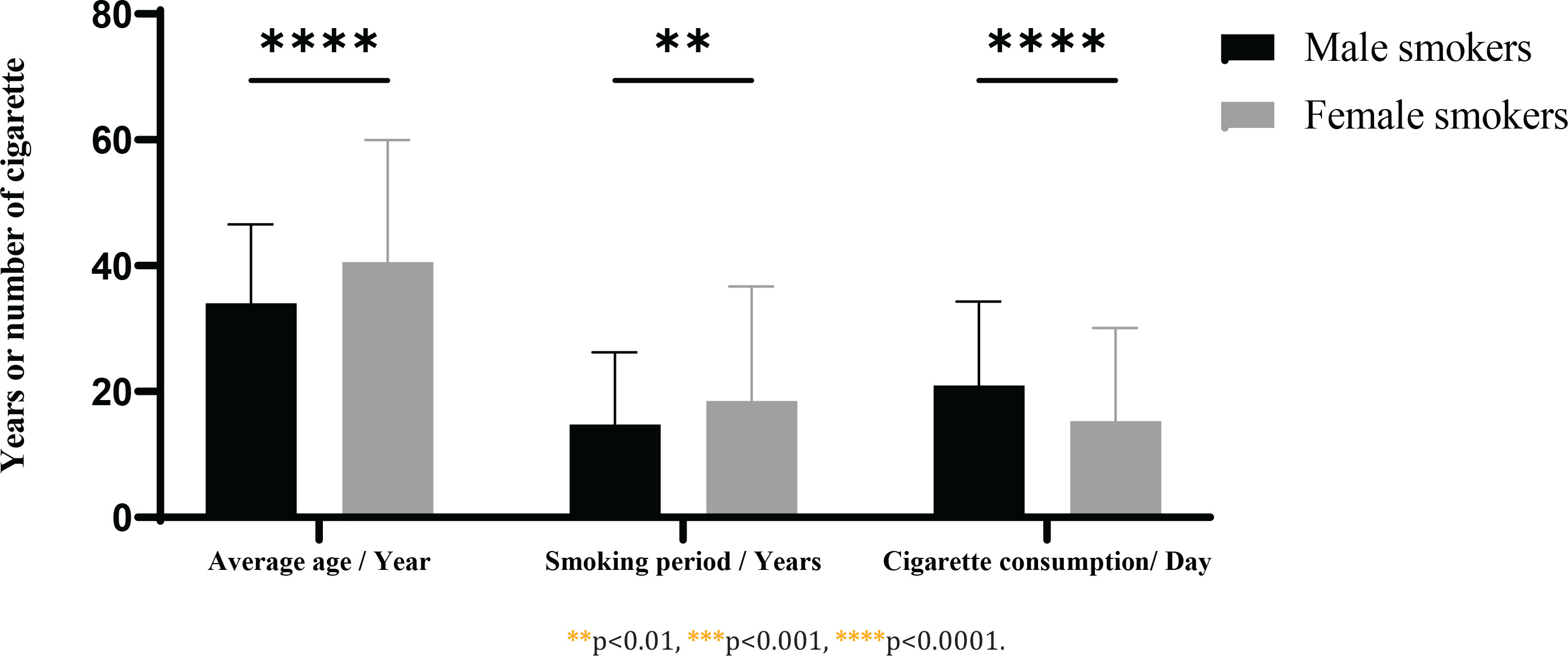
The mean age of female smokers (40.3 ± 19.3 years) was significantly (p<0.0001) higher than that of male smokers (34.0 ± 12.5 years). In addition, the smoking duration of females (18.5 ± 18.2 years) was longer than that of males (14.8 ±11.5 years) (p<0.002). However, males consumed more cigarettes daily (21.0 ± 13.5) than females (15.0 ± 14.7) (p<0.0001) (Figure 1).
Figure 1
Iraqi smokers’ average age (in years, y-axis); smoking period (in years, y-axis) and daily cigarette consumption (number of cigarettes per day, y-axis), by gender, Iraq, August to November 2021 (N=13142)
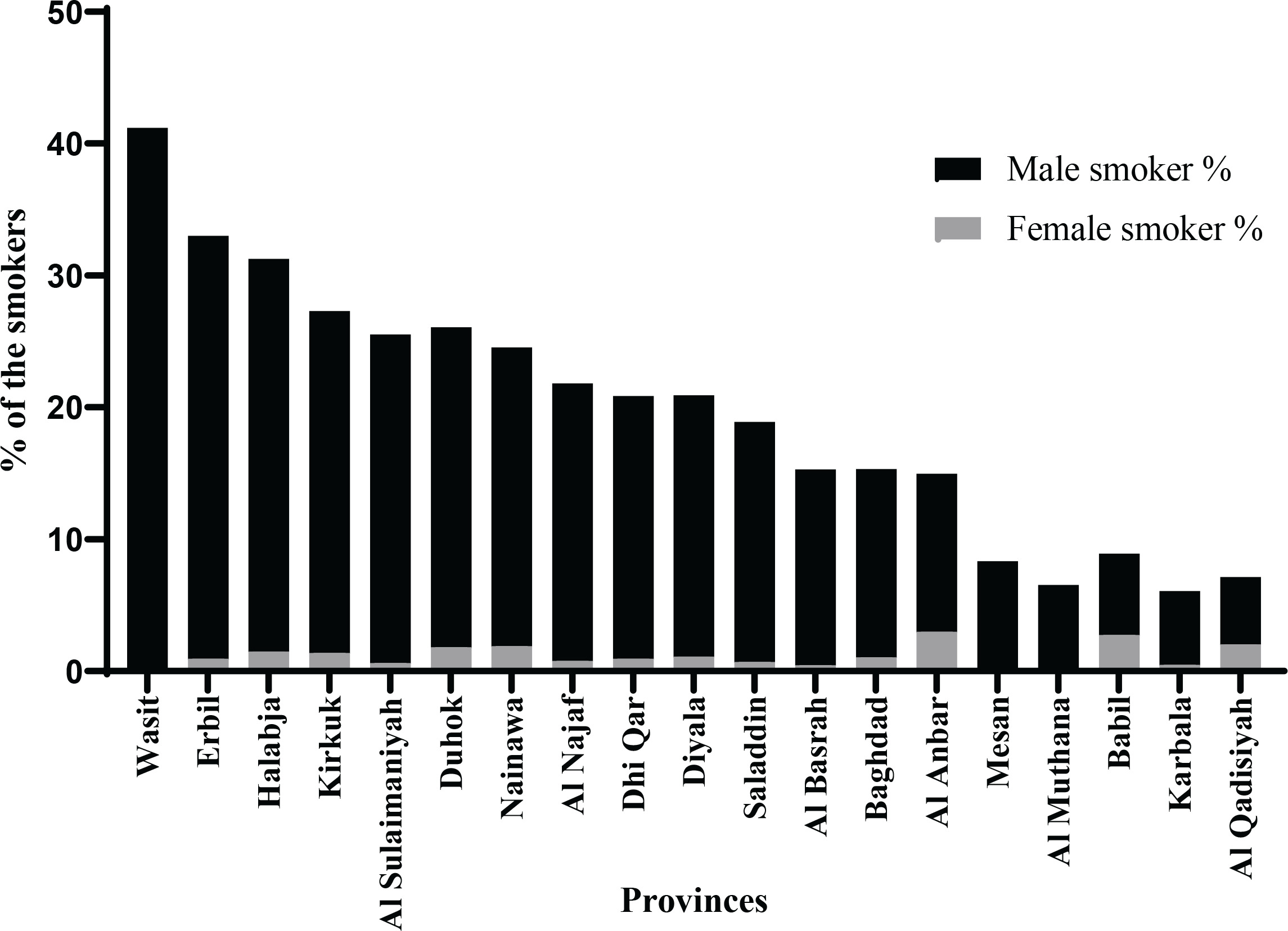
Wasit province had the highest smoking rate (47.1%), followed by Erbil (32.9 %), Halabja (31.3 %), Duhok (26.0%), Nainawa (25.9%) and Al-Sulaimaniyah (25.5%). In contrast, Mesan had the lowest smoking rate (8.3%), followed by Al-Qadisiyah (9.1%), Babil (10.8%), Al-Muthana (10.9%) and Karbala (11.4%) (Figure 3). Males from Wasit had the highest smoking rate (53.3%), with high rates also in Halabja (40.2%), Dhi Qar (40.1%), Erbil (38.5%), Duhok (35.4%) and Kirkuk (34.6%). The male smoking rate was lowest for Babil (18.1%), followed by Basrah (22.1%), Muthanah (22.2%), and Misan (23.8%).
Females from Nainawa had the highest smoking rate of 14.3%, which was about 8% higher than the rates for Duhok, Halabja, and Erbil; the smoking rate for females from other Iraqi provinces did not exceed 5% (Figure 2). Interestingly, female smokers were not recorded for Misan, Al Muthanah and Wasit.
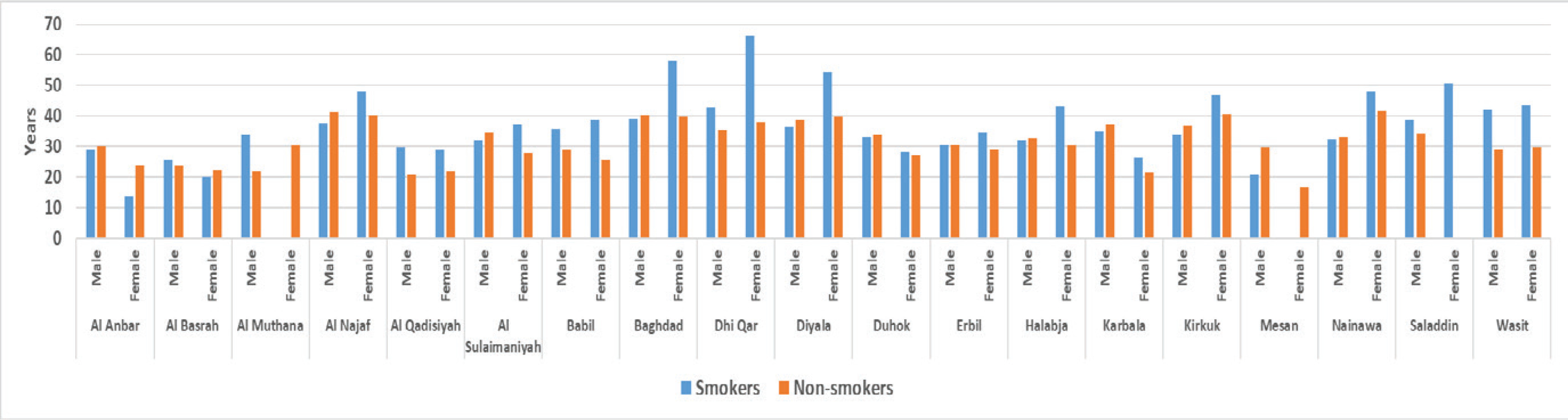
The age of participants in this study ranged from 10 to about 99 years. The average age for both smokers and non-smokers in Misan was the lowest at around 21 years. However, the average age of the participants from Dhi Qar, Baghdad and Saladdin was around 40 years (Figure 3). The average age of male smokers and non-smokers was 21–42 years. However, the range in average age of female smokers was wider, from 13.8 years for Al Anbar to 66.32 years for Dhi Qar, whereas for non-smoking females, the range was between 16.7 years for Mesan and 42.2 years for Saladdin (Figure 3).
Figure 3
Average age of smokers and non-smokers by gender in all Iraqi provinces, August to November 2021(N=13142)
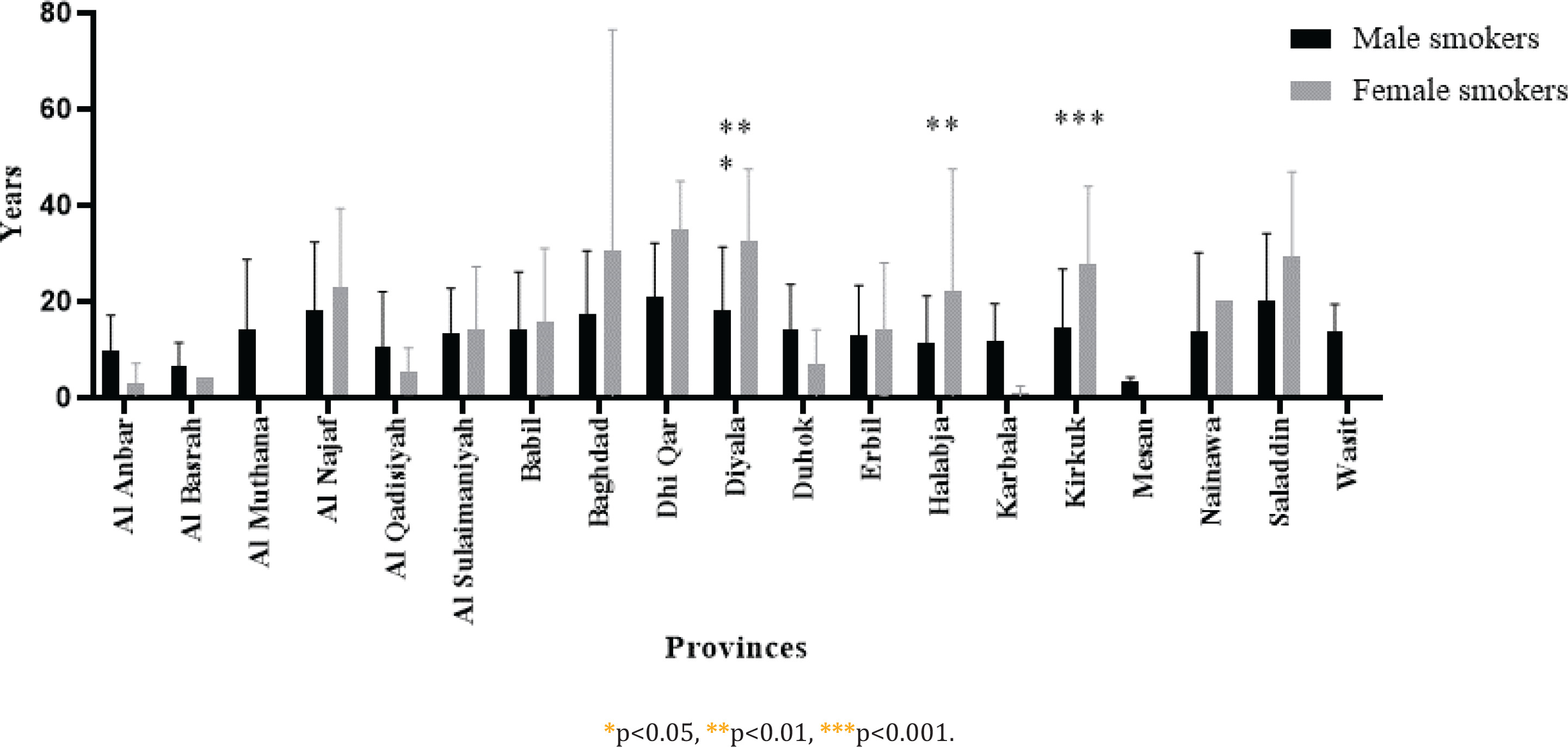
Smokers in Dhi Qar had the longest smoking duration of about 21.3 years, followed by 20.6 years for Saladdin and 19.1 years for Diyala; in contrast, Misan and Basra had the shortest smoking durations of 3.5 and 6.5 years, respectively (Figure 4). Surprisingly, females from most Iraqi provinces had a longer smoking habit, e.g. Dhi Qar (35 years), Diyala (32.7 years), Baghdad (30.8 years), Saladdin (29.3 years), Kirkuk (27.6 years) and Halabja (22 years). On average, the smoking duration of females was 10 years longer than that of males. Dhi Qar recorded the longest smoking habit of 20.9 years for males, followed by Saladdin with 20.3 years (Figure 4).
Figure 4
Smoking duration (years) in each Iraqi province by gender, Iraq, August to November 2021 (N=13142)
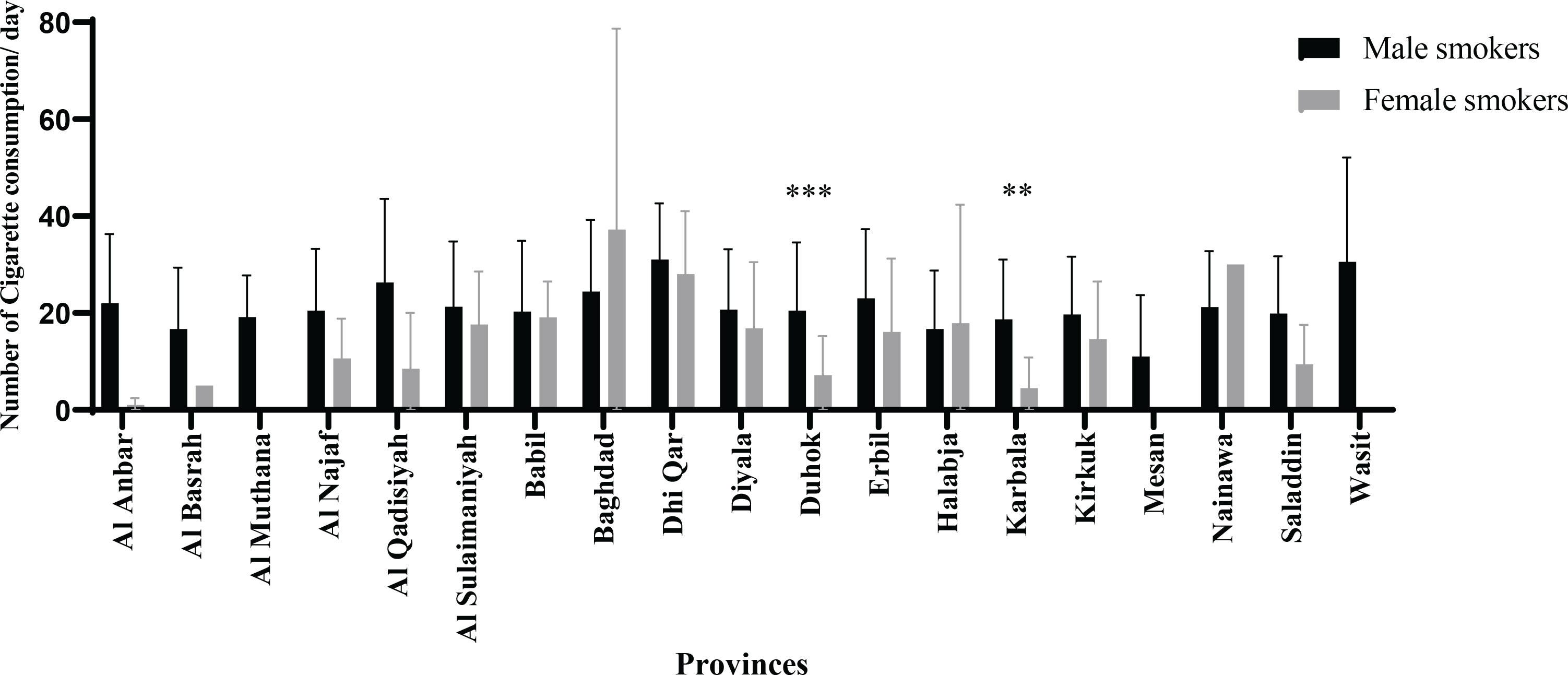
The highest daily cigarette consumption was found in Dhi Qar and Wasit, at 30.5 cigarettes, followed by Baghdad (25.3 cigarettes). In contrast, Misan had the lowest daily cigarette consumption of 11 cigarettes (Figure 5). Iraqi males in all provinces consumed more cigarettes daily than females, except for Baghdad and Nainawa where females’ consumption of cigarettes was one-third higher than males’ consumption. In addition, females from Halabja showed a slightly higher daily cigarette consumption than males (Figure 5).
DISCUSSION
Over the past two decades, a substantial global effort has been made to fight the tobacco epidemic by implementing a set of tobacco control measures to reduce smoking-related diseases and deaths19. Despite these attempts and the many consequences of tobacco use, globally, 942 million men and 175 million women aged ≥15 years are currently smokers20. The smoking rate in the world is about 20% among adults, while it is the highest in Nauru at 48.5%; however, in some countries such as Nigeria and Ghana, the rate is less than 5%21.
This study found that the smoking rate among Iraqi people (13142 participants) is 22.44%, which is lower than that of Turkey (30.5%)22 and higher than that of Iran (17.0%)23, Saudi Arabia (12.2%)24 and the US (14.0%)25. We found that the smoking prevalence among Iraqi males (31.7%) is significantly higher than that among females (3.6%). A similar trend was found in studies related to specific Iraqi sectors26-28.
The percentage of Iraqi male smokers was similar to that found by the WHO (34.1%); however, Iraqi female smokers had half the global smoking rate for women29.
In Iraqi provinces, the smoking rate ranges from 9.1% to 47.1%. In another studies, the percentage of smokers exceeds 30% of the population in Iraq30. However, a low percentage of 21% was found among medical students at three different medical colleges in Baghdad31.
A similar range in the rate (2.4–52.3%) was also found for Saudi Arabia32. In comparison, cigarette use among US adults is 7–24%33. Smoking prevalence among Iraqi males ranges from 18.1 to 40.2%, while for females it is 5.23 to 14.3%. The disparities in smoking rates between men and women revealed in our study are well documented in this part of the world34. In Iran, compared to female participants, the prevalence of smoking among males was seven-fold higher and males started about four years earlier35. In the US, 15.3% of males smoked, a rate only 2.6% higher than that for females25. In the UK, 16.5% of men smoked compared to 13.0% of women; in general, 14.7% of people aged ≥18 years smoked cigarettes in 201836.
According to the US Centers for Disease Control and Prevention (CDC), only around 8% of people aged 18–24 years smoke cigarettes at present, compared to 17% of people aged 25–44 years and 45–64 years, and about 8.2% for those aged ≥65 years21. In addition, in the UK those aged 25–34 years had the greatest percentage (19.2%) of current smokers36. However, we can make only a limited comparison with these rates because the male and female participants in our study were aged between 13.8 and 66.3 years.
Approximately 19% of adults in the world currently smoke cigarettes. In recent years, the percentage of adults who smoke tobacco has decreased, and this trend is expected to continue. According to predictions, only 17% of the world’s population would use tobacco by 2030, down from 21% in 201537.
The smoking habit is not a single behavior, it consists of multiple biological and cultural components38. Overall, tobacco use has been associated with many factors, including social status, education level, age, employment, income level, marital status, psychological status and religious beliefs39. Governments across the globe have attempted to minimize the smoking rate through regulation. Recently, New Zealand approved a tobacco ban for the new generation – from 2022, people aged ≤14 years will never be legally able to buy tobacco40.
In this study, the smoking rate is variable and the smoking habit fluctuates across Iraqi provinces; for example, the range in smoking duration across provinces is 3.5–21.3 years. Surprisingly, women in the majority of Iraqi provinces had a longer smoking habit than men, from 20.3 to 35 years. In this study, the mean age of female smokers was higher. This agrees with the results of John et al.41 which indicate that the proportion of current smokers among females is higher than that among males aged >50 years.
In 2012, the average daily cigarette consumption was <10 in 34 nations, 10–20 in 78 countries, and >20 in 75 countries11. Adults who smoke between one and four cigarettes per day will pass away from various smoking-related diseases as well as from other causes42. In Iraqi provinces, the highest average daily cigarette consumption was 30.5 cigarettes per day and the lowest was 11 cigarettes per day. In general, Iraqi males in all provinces consumed more cigarettes daily than females. Our results show that Iraqi males smoke a high number of cigarettes compared to females as also shown by a study of smokers from Italy and Germany43 which found that male smokers started to smoke earlier and consumed more cigarettes.
Limitations
Several limitations should be taken into account when interpreting the results. There is the possibility of response bias due to the nature of the data reported by the participants. Participants may have incompletely reported or over-reported their smoking habits due to social desirability bias. Individuals sometimes provide responses that they believe are more socially acceptable. Moreover, due to its web-based structure and dissemination of the questionnaire via social media, it is more likely that younger, higher educated participants would participate and hence the final sample may not be generalizable to the exact populational synthesis of Iraq.
CONCLUSIONS
Our study revealed significant gender and regional disparities in smoking rates and behaviors. Additionally, the data highlight significant differences in smoking durations and daily cigarette consumption across provinces. These findings underscore the need for targeted smoking cessation programs that consider both gender and regional differences to effectively address and reduce smoking rates in Iraq. Further studies with random sampling are needed to corroborate these findings.